
When your kidneys aren’t working right, fluid doesn’t just disappear-it builds up. That’s edema. And in chronic kidney disease (CKD), it’s not just swollen ankles. It can be puffy eyes in the morning, a tight belly, or shoes that no longer fit. This isn’t normal aging. It’s your body screaming that it’s holding onto too much salt and water because your kidneys can’t keep up.
Why Edema Happens in CKD
Your kidneys filter about 120-150 quarts of blood every day. They remove waste, balance electrolytes, and control how much fluid stays in your body. When kidney function drops-especially below an eGFR of 60 mL/min/1.73m²-this system breaks down. Sodium sticks around. Water follows sodium. And suddenly, fluid leaks out of your blood vessels into your tissues. This isn’t random. It’s predictable. In stages 3 to 5 of CKD, you’re most likely to see swelling in your legs, feet, and ankles. But it can also show up around your eyes, in your abdomen (ascites), or even in your lungs. The reason? Your kidneys can’t excrete enough sodium. That pushes up blood pressure inside your capillaries. Fluid gets squeezed out into the spaces between cells. And once it’s there, it doesn’t easily go back.Diuretics: The First Line of Defense
Diuretics are the go-to medicine for pulling fluid out. But not all diuretics are the same. And choosing the wrong one can do more harm than good. If your eGFR is below 30, loop diuretics like furosemide, bumetanide, or torsemide are your best bet. These work on the loop of Henle, the part of the kidney that handles the bulk of sodium reabsorption. A typical starting dose of furosemide is 40-80 mg daily. If that doesn’t cut it, doctors may bump it up by 20-40 mg every few days-sometimes all the way to 320 mg. That’s a lot. And it’s not without risk. For people with milder CKD (eGFR above 30), thiazide diuretics like hydrochlorothiazide can still work. But here’s the catch: when both loop and thiazide diuretics are used together-called sequential nephron blockade-it can clear fluid faster. That’s great… until it isn’t. Studies show this combo increases the risk of acute kidney injury by 23%. And over time, people on diuretics lose kidney function faster-on average, 3.2 mL/min/1.73m² per year-compared to 1.7 mL/min/1.73m² in those not on diuretics. Spironolactone is another option, especially if you also have heart failure. It blocks aldosterone, a hormone that makes your body hold onto sodium. But here’s the danger: it can spike potassium levels. In advanced CKD, over 25% of patients on spironolactone end up with dangerous hyperkalemia. That’s why it’s not a first choice unless you’re closely monitored. And now, there’s a new tool: injectable furosemide. Approved by the FDA in March 2025, it’s designed specifically for CKD patients with eGFR under 15. In trials, it cleared fluid 38% better than oral pills. For someone who’s vomiting, not absorbing meds, or too swollen for pills to work, this is a game-changer.Salt Restriction: The Foundation No One Wants to Talk About
You can take all the diuretics in the world. But if you keep eating salt, the fluid will come right back. The National Kidney Foundation says you need to limit sodium to 2,000 mg per day-or even 1,500 mg if you’re in stage 4 or 5 CKD. That’s less than a teaspoon of salt. Sounds simple? It’s not. Most sodium doesn’t come from the salt shaker. It comes from bread (two slices = 300-400 mg), canned soup (one cup = 800-1,200 mg), deli meats (two ounces = 500-700 mg), and frozen meals. Even yogurt and fruit juice have hidden sodium. And don’t forget: fluid counts too. Soups, broths, ice cream, and watermelon all add up. In advanced CKD, total fluid intake often needs to be capped at 1,500-2,000 mL per day. A 2022 study from the American Kidney Fund found that people who stuck to a 2,000 mg sodium limit for just 2-4 weeks saw a 30-40% drop in swelling-even without diuretics. But here’s the problem: 68% of CKD patients say they can’t stick to it. Taste is the biggest issue. Social situations come second. And low-sodium food options? Still hard to find. Real change needs more than a handout. It needs a renal dietitian. Three to four sessions on reading labels, cooking without salt, and finding alternatives make all the difference. Without that support, most people fail.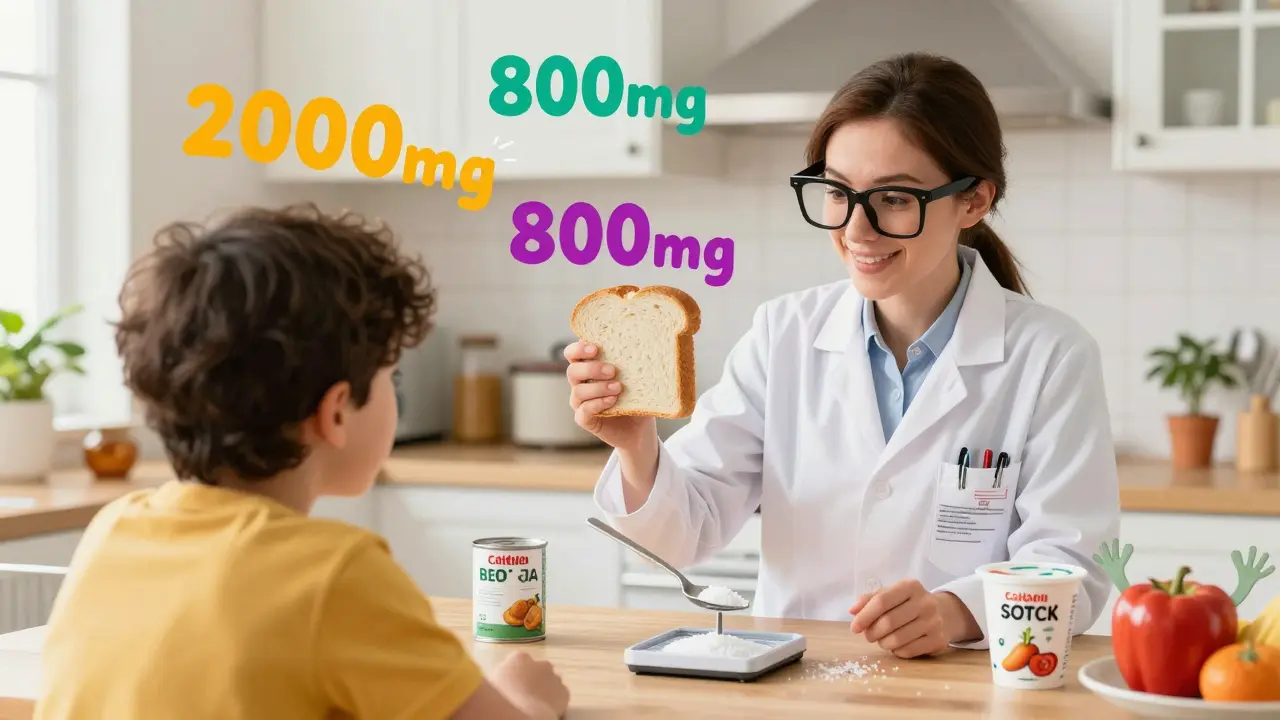
Compression Therapy: More Than Just Stockings
Diuretics and salt control tackle the root cause. But compression therapy tackles the symptom-right where it hurts. Graduated compression stockings (30-40 mmHg at the ankle) are the gold standard for leg swelling. They squeeze from the foot up, pushing fluid back toward your heart. Studies show they can reduce leg volume by 15-20% in just four weeks. But here’s the kicker: only 38% of people wear them consistently beyond three months. Why? They’re uncomfortable. Hard to put on. And they irritate the skin. Elevating your legs above your heart for 20-30 minutes a few times a day helps too. It’s simple. Free. And effective-cutting swelling by 25-30% in many cases. Walking matters. A 2021 Cochrane review found that 30 minutes of walking five days a week improved edema control by 22% compared to just resting. Movement isn’t just good for your heart-it helps your lymphatic system drain fluid. For severe cases, especially with nephrotic syndrome, intermittent pneumatic compression devices (IPCs) are used. These are machines that wrap around your legs and inflate in cycles, mimicking muscle movement. One study showed they reduced leg circumference 35% more than regular stockings alone.The Balancing Act
There’s no perfect answer. Every treatment has trade-offs. Dr. David Wheeler, who helped write the KDIGO guidelines, says the window for diuretics in advanced CKD is narrow. Push too hard, and you risk crashing your kidneys. But leave fluid in, and your risk of death goes up 28%. The numbers don’t lie. People with persistent edema have higher hospitalization rates, worse heart function, and shorter lifespans. Yet, aggressive diuresis can lead to dizziness, cramps, low blood pressure, and even kidney failure. The sweet spot? Slow, steady fluid removal. Aim for 0.5-1.0 kg (1-2 pounds) of weight loss per day. Too fast? You’ll dehydrate your kidneys. Too slow? Fluid keeps building. And here’s the real secret: it’s not one thing. It’s the combo. A Mayo Clinic registry found that patients who got care from a team-nephrologist, dietitian, physical therapist-had a 75% success rate in controlling edema within eight weeks. Those with standard care? Only 45%.
What You Can Do Today
You don’t need to fix everything at once. Start here:- Check your sodium intake. Use an app like MyFitnessPal to track every bite for three days. You’ll be shocked.
- Swap one high-sodium food for a low-sodium version. Try fresh chicken instead of deli meat. Cook your own soup instead of buying canned.
- Elevate your legs for 20 minutes after dinner. Use pillows. No fancy gear needed.
- Walk for 15 minutes after lunch. Even if you’re tired. Movement is medicine.
- Ask your doctor about a referral to a renal dietitian. It’s covered by Medicare and most insurers.
When to Call Your Doctor
Call immediately if you notice:- Sudden weight gain of more than 2 pounds in 24 hours
- Shortness of breath, especially when lying down
- Swelling that spreads to your abdomen or hands
- Dizziness, confusion, or very little urine output
What’s Coming Next
The future of edema management in CKD is getting smarter. The NIH’s FOCUS trial, ending in late 2025, is testing whether using bioimpedance spectroscopy (BIS) to measure fluid levels in real time can guide diuretic dosing better than guesswork. Early results show 32% fewer hospital visits. New drugs like vaptans are being studied, but early trials hit roadblocks due to liver damage. For now, the best tools are still the ones we’ve had for decades-just used better. The message is clear: edema in CKD isn’t something to ignore. It’s not just swelling. It’s a sign your body is under stress. And managing it isn’t about one pill or one diet. It’s about a plan-tailored, consistent, and supported. You can control this. But you have to play the long game.Can edema in CKD go away on its own?
No. Edema in chronic kidney disease doesn’t resolve without intervention. It’s caused by the kidneys’ inability to remove sodium and water, which won’t fix itself as kidney function declines. Left untreated, it worsens and increases the risk of heart failure, hospitalization, and death. Management requires a combination of salt restriction, diuretics, and mechanical support like compression.
Are diuretics safe for long-term use in CKD?
Diuretics can be safe when used carefully, but they’re not risk-free. Long-term use is linked to faster kidney function decline-about 3.2 mL/min/1.73m² per year compared to 1.7 in non-users. They also raise the risk of low blood pressure, muscle cramps, and electrolyte imbalances. The key is using the lowest effective dose, monitoring kidney function and potassium levels regularly, and combining them with salt restriction to reduce dependency.
How much salt should someone with CKD eat daily?
The National Kidney Foundation recommends no more than 2,000 mg of sodium per day for CKD patients with edema. For those in stage 4 or 5, the target drops to 1,500 mg per day. That’s less than a teaspoon of table salt. Most sodium comes from processed foods-not the salt shaker-so reading labels and cooking at home are essential. Even small changes, like switching from canned soup to low-sodium versions, can make a big difference.
Do compression stockings really help with kidney-related swelling?
Yes. Graduated compression stockings (30-40 mmHg) help push fluid back toward the heart, reducing leg swelling by 15-20% in as little as four weeks. They’re especially helpful for people who can’t take high doses of diuretics or need extra support between doses. However, many patients stop using them because they’re uncomfortable or hard to put on. Working with a physical therapist to find the right fit and learn proper donning techniques improves adherence.
What’s the fastest way to reduce edema in CKD?
The fastest results come from combining treatments: a low-sodium diet, a loop diuretic like furosemide, and leg elevation. For advanced cases, intravenous furosemide (approved in March 2025) can clear fluid 38% faster than oral pills. Weight loss should be gradual-0.5 to 1.0 kg per day-to avoid kidney damage. Rapid fluid removal can cause low blood pressure or acute kidney injury, so speed isn’t always better.
Can I stop taking diuretics if I cut out salt?
Some people with early-stage CKD (stages 1-3) can reduce or even stop diuretics with strict salt restriction and lifestyle changes. But in stages 4-5, the kidneys are too damaged to handle fluid balance on their own. Even with perfect diet adherence, most will still need some diuretic support. Never stop or adjust diuretics without your doctor’s guidance-sudden changes can cause dangerous fluid buildup or dehydration.
Why does my swelling get worse at night?
Fluid redistributes when you lie down. During the day, gravity pulls fluid into your legs. At night, when you’re horizontal, that fluid moves back into your bloodstream, making your kidneys work harder. If they can’t keep up, fluid leaks into tissues, especially around your eyes and face. This is why morning puffiness is common in CKD. Elevating your legs during the day and limiting fluids in the evening can help.
Is there a cure for edema in CKD?
There’s no cure for edema in CKD unless the underlying kidney disease is reversed-which rarely happens. But edema can be controlled. With the right mix of diet, medication, and compression therapy, most people can live comfortably without hospitalizations. The goal isn’t to eliminate swelling entirely-it’s to keep it at a level that doesn’t affect your breathing, mobility, or quality of life.




Linda O'neil
January 27, 2026 AT 15:36Just wanted to say this post saved my life. I was in stage 4 CKD and thought swelling was just part of getting older. Started cutting salt, walking after dinner, and using my compression stockings every day. Lost 8 pounds in 3 weeks without touching diuretics. You’re not alone - this stuff works if you stick with it.
Also, the renal dietitian referral? Do it. Mine helped me find cheap low-sodium frozen meals. Who knew you could eat like a human and still protect your kidneys?
Robert Cardoso
January 28, 2026 AT 20:48Let’s be real - diuretics are a band-aid on a gunshot wound. The real problem is the medical system’s obsession with pills over prevention. You want to fix edema? Stop treating symptoms and start treating the root: processed food, corporate lobbying, and doctors who don’t know how to cook.
And don’t get me started on the FDA approving injectable furosemide. That’s not innovation - that’s corporate profit dressed up as progress. The same companies selling you the pills also sell the salt-laden food that caused this in the first place.
Irebami Soyinka
January 28, 2026 AT 22:04Wow, America still thinks a teaspoon of salt is the problem? In Nigeria, we don’t even know what ‘sodium’ means - we just know that when your body swells, you go to the herb doctor, not the pill pusher.
This whole post reads like a pharmaceutical ad with footnotes. Diuretics? Compression socks? Please. My uncle had CKD for 12 years. He drank bitter leaf tea, walked barefoot on grass every morning, and never saw a doctor. He’s still alive. You think your science is better? Maybe you’re just louder.
doug b
January 30, 2026 AT 03:14Start small. One change. That’s all you need. Swap the canned soup for homemade. Walk for 10 minutes. Elevate your legs while watching TV.
You don’t have to be perfect. You just have to show up. I’ve seen people turn things around with just these three things. Your body hears you - even when you think it’s too late.
Chris Urdilas
January 30, 2026 AT 07:02So let me get this straight - we’re being told to eat less salt, take more pills, wear uncomfortable socks, and walk more… all while the FDA approves a new injectable version of a 70-year-old drug?
That’s not medicine. That’s a hamster wheel with a fancy label. And the real kicker? The ‘team-based care’ that works 75% of the time? Most people can’t even get a 15-minute appointment with a nephrologist. This post is brilliant - but it’s written for people who already have access to everything. What about the rest of us?
Also, ‘move more’ is the most overused phrase in medicine. Try telling that to someone who’s too tired to lift their leg because their kidneys are failing.
Phil Davis
January 31, 2026 AT 11:24Interesting how everyone’s talking about diuretics and salt like they’re the heroes here.
Meanwhile, no one mentions that the same people pushing these guidelines also profit from the very products that cause the problem. Salt is cheap. Diuretics are expensive. Compression stockings? Insurance barely covers them.
And yet, we’re supposed to believe this is about health, not economics.
Also - ‘ask your doctor for a referral’? Sure. If your doctor isn’t already overwhelmed, underpaid, and trained to write scripts, not teach life skills.
Jeffrey Carroll
February 1, 2026 AT 00:10This is one of the most thoughtful, evidence-based summaries I’ve read on CKD edema management. The balance between clinical reality and patient experience is rare. I appreciate the emphasis on the team approach - nephrologists alone cannot solve this. Dietitians, PTs, and nurses are the unsung heroes here.
Also, the point about fluid intake being part of sodium restriction is critical. Many patients focus only on salt and ignore soups, broths, and even fruit. That’s where the real slip-ups happen.
Thank you for not sugarcoating the risks of diuretics. We need more honesty, not just hope.
Mel MJPS
February 1, 2026 AT 16:42I’ve been on dialysis for 3 years. Edema was my worst enemy until I started wearing my compression socks every day. They’re a pain to put on, but I do it while watching my morning show. Now I can walk to the mailbox without feeling like I’m carrying two water balloons.
Also - I started using the MyFitnessPal app like you said. Turned out I was eating 5,000 mg of sodium a day. I didn’t even realize. Now I cook everything from scratch. My husband hates it. I don’t care. I’m alive.
SRI GUNTORO
February 3, 2026 AT 11:21Of course you recommend salt restriction. Because obviously, the poor person with CKD is the one who chose to eat processed food. Maybe if they hadn’t been born into poverty, they’d have had time to read labels and cook from scratch.
But no - the problem is always the patient’s willpower. Never the system that makes unhealthy food cheaper than vegetables.
And don’t get me started on ‘walking more.’ Tell that to the single mom working two jobs and caring for her diabetic mother. Your ‘simple solutions’ are just another way to blame the victim.
Rhiannon Bosse
February 5, 2026 AT 02:51Wait - so the FDA approved injectable furosemide in March 2025… but no one’s talking about how the same company that makes it also owns the patent on the salt substitute that causes kidney damage in 1 in 4 patients?
And the ‘FOCUS trial’? That’s just a cover for Big Pharma to get more data before pushing another $12,000/month device on Medicare.
And why is no one asking why 68% of patients can’t stick to low-salt diets? Because they’re being fed poison by the same corporations that fund the NKF.
Wake up. This isn’t medicine. It’s a pyramid scheme with stethoscopes.
Timothy Davis
February 5, 2026 AT 10:03Let’s debunk the myth: diuretics don’t cause faster kidney decline - the disease does. The correlation is misinterpreted. Studies show patients on diuretics are sicker to begin with - that’s why they’re prescribed them. The diuretic isn’t the cause; it’s the marker.
Also, the 3.2 mL/min/year decline? That’s from observational data with zero control for comorbidities. Anyone who cites this as proof diuretics are harmful is either misinformed or lying.
And compression therapy? It’s not magic. It’s physics. If you’re not using graduated compression above 30 mmHg, you’re wasting time. And if you’re not elevating legs at 30 degrees, you’re doing it wrong.
Also - ‘eat fresh chicken’? Who has time for that? Most CKD patients are elderly, disabled, or on fixed incomes. This post reads like a wellness influencer’s dream, not a clinical guide.
James Dwyer
February 5, 2026 AT 14:42My dad had CKD. He hated diuretics because they made him dizzy. But he loved his compression socks. He’d put them on every morning like armor. Said they made him feel like he still had control.
He didn’t live to see the injectable furosemide. But if he had, I think he’d have said: ‘Just don’t let them make me a lab rat.’
This post? It’s the kind of thing I wish I’d had when he was sick. Thank you.
jonathan soba
February 5, 2026 AT 14:46Interesting how the author conveniently omits that loop diuretics are less effective in CKD beyond stage 4 due to tubular atrophy - yet still recommends up to 320 mg of furosemide. That’s not clinical wisdom. That’s desperation dressed as protocol.
And the ‘team-based care’ success rate? That’s only possible in academic centers with research funding. In rural America? You’re lucky if you get a phone call from your nephrologist every six months.
This isn’t a guide. It’s a fantasy.